Microsurgical Vasectomy Reversal
Robert U. Finnerty M.D. FACS
 For many reversal surgeons, there is no choice in the type of reversal surgery performed. Those trained only in non-microsurgical techniques, or with little or no training or experience in microsurgical techniques, especially epididymal repair, will only perform a vas-to-vas repair (VV). If you are fortunate enough to have no epididymal obstruction, and the surgeon has adequate training in microsurgery, you may have a reasonable chance for a successful outcome.
For many reversal surgeons, there is no choice in the type of reversal surgery performed. Those trained only in non-microsurgical techniques, or with little or no training or experience in microsurgical techniques, especially epididymal repair, will only perform a vas-to-vas repair (VV). If you are fortunate enough to have no epididymal obstruction, and the surgeon has adequate training in microsurgery, you may have a reasonable chance for a successful outcome.
However, experience has shown that a significant percentage of men will develop epididymal obstruction after vasectomy — even those who are a relatively short time after vasectomy. Surgeons experienced in microsurgical reconstruction and epididymal repair (VE).
In the past, success rates for epididymal repairs were relatively poor, even with microsurgery, and every effort was made to avoid this procedure where possible. With much improved success rates, many of these previously-unrecognized epididymal blockages can be addressed successfully. Furthermore, successful epididymal repair is often associated with significantly improved sperm quality and fertility.
There is no reliable way to determine the presence of epididymal obstruction before surgery. Statistics such as time post vasectomy may indicate a higher chance of its occurrence, but on an individual basis, this can only be determined at surgery.
 At the time of reversal surgery, the vasectomy site is removed, which allows fluid to be expressed from the testicular end of the vas. In the past, the presence of any sperm or sperm parts was thought to indicate that no obstruction was present. Even men with no sperm — if the fluid appearance was clear — were considered to be unobstructed.
At the time of reversal surgery, the vasectomy site is removed, which allows fluid to be expressed from the testicular end of the vas. In the past, the presence of any sperm or sperm parts was thought to indicate that no obstruction was present. Even men with no sperm — if the fluid appearance was clear — were considered to be unobstructed.
Experience has shown that the incidence of obstruction is very high in men who have no sperm (regardless of fluid appearance), sperm parts only, or inactive (non-motile) sperm with fluid which appears thick or creamy.
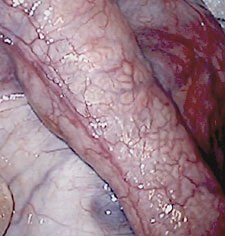 Direct inspection of the epididymis is necessary in all such questionable situations. The point of blockage can generally be detected by the appearance of the epididymal tubules (which can be seen through the thin, translucent outer layer of the epididymis), whether the tubules are distended above a point and decompressed below, and by testing the epididymal fluid directly for the presence of active sperm.
Direct inspection of the epididymis is necessary in all such questionable situations. The point of blockage can generally be detected by the appearance of the epididymal tubules (which can be seen through the thin, translucent outer layer of the epididymis), whether the tubules are distended above a point and decompressed below, and by testing the epididymal fluid directly for the presence of active sperm.
Sperm flows from the testes, into the efferent ducts, and down the epididymis toward the vas. Above the obstruction, the epididymal tubules will be distended, and often have a creamy fluid seen through the wall of the tubule. Below the obstruction, the tubules are decompressed and often more translucent. These transition zones help identify points of obstruction (of which there may be more than one), but specific testing for sperm in the epididymal fluid (by opening the tubule, and examining the fluid under a lab microscope) must be preformed to ensure the obstruction is bypassed.